Case Review (Open Fracture)
CC/HPI: 60 year old female presents to TUH emergency department via EMS after a "slip and fall" accident. Pt states she was cleaning the kitchen when she fell and twisted her Right ankle. She felt immediate pain and saw that her skin had "ripped" open. It occurred two hours ago. Her Tetanus status is up to date. Antibiotics were immediately started in the ER.
What is your next action?
Always take a detailed history and physical.
PMH: IDDM, COPD (on home O2 2L), CVA 2009 (not on coumadin), HTN, hyperlipidemia
Meds: Plavix, Lisinopril, Insulin, lipitor
Allergies: none
ROS: negative for fevers, chills, nausea, vomiting, chest pain, SOB, Headache, dizziness
FH: positive for DM, father died of MI
SH: denies EtOH, drug use, tobacco
Vitals: Tcur 98.7 P90 R22 BP 160/70 99 2L
Physical Exam:
Vascular: R DP Pulse palpable, PT dopplerable signal, CFT to digits X R5 digits < 3secs
Neuro: Gross sensation intact to digits x 5
Ortho: gross clinical dislocation of R ankle joint
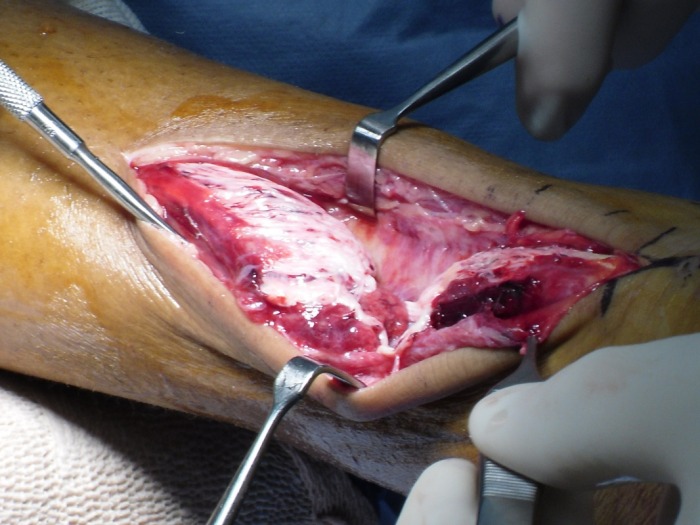
Derm: Anterior and medial laceration 12 cm in length with TA tendon exposed w/ copious amounts of dried hematoma


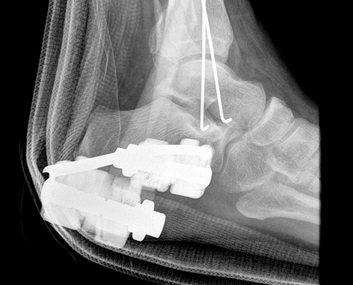
Xrays Performed


Labs
Procedure Performed: Closed Reduction w/ Conscious Sedation w/ Post Reduction Xrays


Pt taken to OR immediately for Delta Frame Application and Wound Washout!

Intraop- Wound was primarily closed with 2-0 nylon suture and an incisional Wound VAC was placed.
Questions to Review
1. This laceration/wound was primarily not left open. What does the golden period refer to?
2. This patient had her tetanus status up to date. Review when to administer tetanus toxoid and tetanus Immunoglubolin for a tetanus prone wound versus non tetanus prone wound. What are the dosages?
3. This patient had a CVA (cerebral vascular accident) back in 2009 and finished her dosing of coumadin. If this pt was on coumadin and her INR was at 3.0, what could have been done to immediately lower the INR. At what value do you want the INR to be for surgery?
4. Initial Xrays showed fracture/dislocation of the R ankle joint. What is the Classification of this Open Fracture considering that the blood supply is intact and that there is a enough soft tissue to close the wound? What is the Ankle Fracture Classification for this patient?
5. Closed Reduction was performed at Bedside with conscious sedation. What are the 3 steps to closed reduction? **In open fractures, you never increase the deformity as you will make the soft tissue defect worse**
6. Conscious sedation was performed. Name as many drugs that could possibly be given during consious sedation. What are the reversal agents for narcotic and benzodiazepine overdose?
7. This is a surgical emergency because it is a limb threatening injury. What are some other surgical emergencies in the podiatric surgical field? In an open fracture, is it more important to stabilize the soft tissue or to fixate the bone?
8. Antibiotics were immediately started on this patient. According to the Gustillo Anderson Classification what antibiotics should be started on this patient? Are these antibiotics therapeutic or prophylactic?
9. What is a delta frame? What is the purpose of the delta frame? Where are the pins inserted for a delta frame?
10. K-wires were used to fixate the medial malleolar fracture through the primary wound to help stabilze the ankle, however the fibular fracture was not stabilized at this time to avoid making an additional incision. Classically what is more important to reducing an ankle joint, fixating the fibular fracture or medial malleolar fracture.
11. An incisional Wound VAC was placed on the primarily closed wound. What data supports applying a VAC postop. Is it applied to every patient that receives surgery? How many days postop is the wound vac left on? Once again what is the Golden Period?
2. This patient had her tetanus status up to date. Review when to administer tetanus toxoid and tetanus Immunoglubolin for a tetanus prone wound versus non tetanus prone wound. What are the dosages?
3. This patient had a CVA (cerebral vascular accident) back in 2009 and finished her dosing of coumadin. If this pt was on coumadin and her INR was at 3.0, what could have been done to immediately lower the INR. At what value do you want the INR to be for surgery?
4. Initial Xrays showed fracture/dislocation of the R ankle joint. What is the Classification of this Open Fracture considering that the blood supply is intact and that there is a enough soft tissue to close the wound? What is the Ankle Fracture Classification for this patient?
5. Closed Reduction was performed at Bedside with conscious sedation. What are the 3 steps to closed reduction? **In open fractures, you never increase the deformity as you will make the soft tissue defect worse**
6. Conscious sedation was performed. Name as many drugs that could possibly be given during consious sedation. What are the reversal agents for narcotic and benzodiazepine overdose?
7. This is a surgical emergency because it is a limb threatening injury. What are some other surgical emergencies in the podiatric surgical field? In an open fracture, is it more important to stabilize the soft tissue or to fixate the bone?
8. Antibiotics were immediately started on this patient. According to the Gustillo Anderson Classification what antibiotics should be started on this patient? Are these antibiotics therapeutic or prophylactic?
9. What is a delta frame? What is the purpose of the delta frame? Where are the pins inserted for a delta frame?
10. K-wires were used to fixate the medial malleolar fracture through the primary wound to help stabilze the ankle, however the fibular fracture was not stabilized at this time to avoid making an additional incision. Classically what is more important to reducing an ankle joint, fixating the fibular fracture or medial malleolar fracture.
11. An incisional Wound VAC was placed on the primarily closed wound. What data supports applying a VAC postop. Is it applied to every patient that receives surgery? How many days postop is the wound vac left on? Once again what is the Golden Period?
Case Review (Achilles Tendon Rupture)
CC/HPI:38 year old male presents to TUH emergency department complaining of severe pain to the posterior L heel and leg. Pt states he was playing basketball about 3 hours ago and as he was running, he heard a “pop” and felt as if someone had just kicked him in the back of the leg. Pt relates he has been seeing a podiatrist the last couple of weeks for serial corticosteroid injections into his left achilles insertion due to inflammation.
What is your next action?
Always take a detailed history and physical.
PMH: none
Med: none
Allergies: none
SH: smokes marijuana two times a day; denies alcohol use
FH: non-contributory
ROS: denies f/c/n/v
Vitals: t: 99.2 hr: 80 resp: 16 bp: 130/70
Physical Exam:
Vascular: L DP/PT pulse palpable; L CFT <3 sec
Neuro: Sensation Intact L
Derm: Edema is noted at the L posterior heel; no open lesions; no signs of clinical infection
Ortho: Pain on palpation at the insertion to 3cms proximal to the L achilles tendon insertion; Palpable gap at about 2cms from the left achilles insertion; L positive Thompson test; Plantarflexory power of L foot is significantly diminished compared to R foot
What is your next action?
X-rays: Lateral view of the left foot shows obliteration of the kager’s triangle and also an abnormality in toygar’s line
What other image modality should you use?
An MRI of the left foot/ankle was performed:
T1: showed a 4cm gap starting from about 2.5cm from the insertion of achilles
T2: showed significant increase in signal intensity at the left achilles tendon at about the visible gap
What is your treatment?
This patient was actually brought to the OR that day for achilles repair using the krackow stitch (review Kessler, Bunnel vs Krackow). It was reinforced with Graftjacket and then the pt was placed in cast with the ankle in a plantarflexory position. One must realize that at that point, the pt was determined to have stable soft tissue of his left posterior heel and leg. Excessive edema or any type of open wound would further complicate the closure of the L Achilles surgical incision and place the patient at a higher risk of dehiscense and possible non-healing of the incision.
If in the ED and the patient had unstable soft tissue, he would have been placed in a Jones compression wrap either with a posterior splint or shell with the ankle at about 20 degrees of plantarflexion. After it was determined that the soft tissue was stable, then surgery could have been performed most likely in an outpatient setting.
What is your next action?
Always take a detailed history and physical.
PMH: none
Med: none
Allergies: none
SH: smokes marijuana two times a day; denies alcohol use
FH: non-contributory
ROS: denies f/c/n/v
Vitals: t: 99.2 hr: 80 resp: 16 bp: 130/70
Physical Exam:
Vascular: L DP/PT pulse palpable; L CFT <3 sec
Neuro: Sensation Intact L
Derm: Edema is noted at the L posterior heel; no open lesions; no signs of clinical infection
Ortho: Pain on palpation at the insertion to 3cms proximal to the L achilles tendon insertion; Palpable gap at about 2cms from the left achilles insertion; L positive Thompson test; Plantarflexory power of L foot is significantly diminished compared to R foot
What is your next action?
X-rays: Lateral view of the left foot shows obliteration of the kager’s triangle and also an abnormality in toygar’s line
What other image modality should you use?
An MRI of the left foot/ankle was performed:
T1: showed a 4cm gap starting from about 2.5cm from the insertion of achilles
T2: showed significant increase in signal intensity at the left achilles tendon at about the visible gap
What is your treatment?
This patient was actually brought to the OR that day for achilles repair using the krackow stitch (review Kessler, Bunnel vs Krackow). It was reinforced with Graftjacket and then the pt was placed in cast with the ankle in a plantarflexory position. One must realize that at that point, the pt was determined to have stable soft tissue of his left posterior heel and leg. Excessive edema or any type of open wound would further complicate the closure of the L Achilles surgical incision and place the patient at a higher risk of dehiscense and possible non-healing of the incision.
If in the ED and the patient had unstable soft tissue, he would have been placed in a Jones compression wrap either with a posterior splint or shell with the ankle at about 20 degrees of plantarflexion. After it was determined that the soft tissue was stable, then surgery could have been performed most likely in an outpatient setting.



Key Points to look up
- What is the typical patient that is usually afflicted with an Achilles tendon rupture?
- This patient had multiple corticosteroid injections into the left heel which predisposed him to Achilles rupture. What other drug/s could also predispose him to rupture?
- What is the Thompson Test?
- What is the watershed zone?
- How does the Achilles tendon receive it’s blood supply?
- What is the classification for Achilles rupture?
- What other surgical treatments can be performed? For larger ruptures?
- What are the borders of Kager’s triangle and what is toygar’s line?
- This patient still had some plantarflexory power of his left foot? How is that possible if he ruptured his Achilles?
- What is the difference between the Kessler, Bunnel and Krackow Stitch?
- Why perform surgery on this patient? What is the general consensus in the literature on the re-rupture rates of conservative treatment versus surgical treatment?
